Testosterone "Within Normal Range" but Still Feeling Off?

“Normal” on a test result isn’t the same as “healthy”
The reference range you see next to your result is a statistical construct, not a health threshold. It’s determined by measuring hormone levels in a population considered representative and excluding the extreme values. Simply put, “normal” describes where most of the tested population falls, not the level below which symptoms appear. These are two different concepts, even though they look identical on paper.
The second issue is technical. Different labs use different testing methods and reference populations, so the same sample might be “normal” in one lab and “below normal” in another. The most accurate method is liquid chromatography coupled with mass spectrometry (LC-MS/MS), but routine diagnostics still rely heavily on cheaper immunoassays, which can be unreliable at low concentrations. This is why comparing a “bare” result to online tables without checking the units and the specific lab’s range is not very reliable.
The Same Number, Different Conclusions, Debate Over the Threshold
Scientific societies disagree on where the deficiency threshold lies. The American Urological Association (AUA) considers total testosterone below 300 ng/dl (approximately 10.4 nmol/l) to be low. The European Association of Urology (EAU), on the other hand, uses a threshold of 12 nmol/l (approximately 3.46 ng/ml, or 346 ng/dl). As a result, a level of 315 ng/dl is deemed "normal" by the AUA but "low" by the EAU. This isn't a lab error, but rather a genuine discrepancy in definitions.
This discrepancy creates what is known as a gray zone, roughly between 8 and 12 nmol/l. It encompasses a significant group of men with symptoms, where the number alone doesn't determine whether intervention is necessary.
Individual variability further complicates the matter. One man with testosterone at 10 nmol/l may exhibit clear symptoms, while another with the same level feels perfectly fine. There is no universal number that means the same for everyone. This is one of the main reasons why diagnoses are not based solely on test results but on those results combined with the clinical picture.

Testosterone Deficiency Thresholds in Selected Guidelines
American Guidelines (AUA). Total testosterone below 300 ng/dl (3.0 ng/ml, approximately 10.4 nmol/l) is considered low, and routine measurement of free testosterone is not required.
European Guidelines (EAU). They use a threshold of 12 nmol/l (3.46 ng/ml, approximately 346 ng/dl) and recommend measuring free testosterone in the grey zone between 8 and 12 nmol/l.
Endocrine Society (endocrinology). Results are interpreted based on the specific method's range, requiring two fasting morning measurements, and free testosterone is measured when SHBG abnormalities are suspected.
Approximate conversion: 1 nmol/l ≈ 0.288 ng/ml ≈ 28.8 ng/dl.
Total Testosterone Is Not the Whole Story: SHBG and Free Testosterone
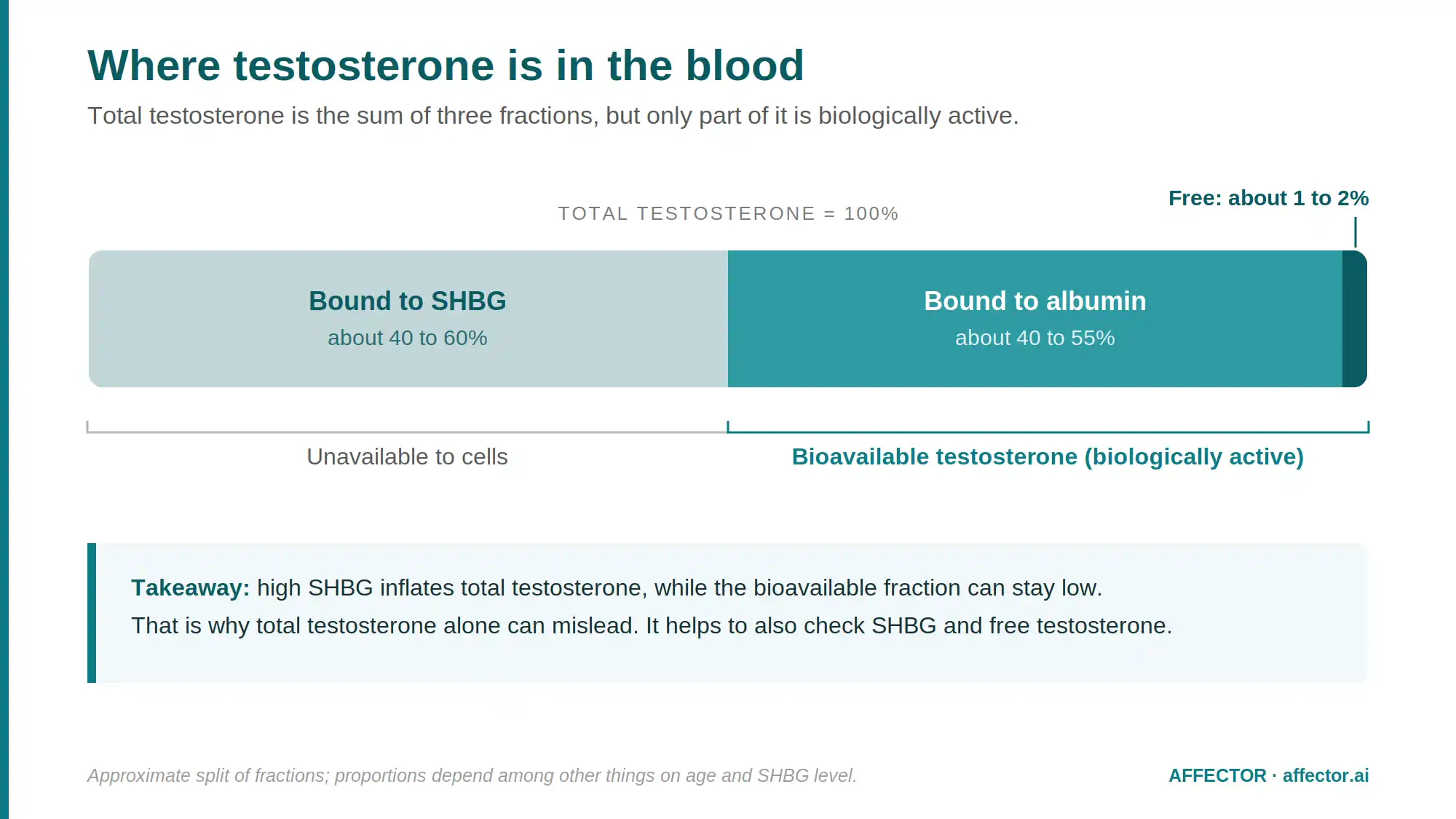
Most circulating testosterone is not available to cells. Between 40 and 60 percent is tightly bound to the carrier protein SHBG (sex hormone-binding globulin), another large portion is loosely bound to albumin, and only a small percentage circulates as free testosterone. The biologically active fractions are the free testosterone and the albumin-bound portion, collectively referred to as bioavailable testosterone. Total testosterone sums everything, including the fraction that is essentially inactive.
This explains one of the most common paradoxes in test results. If SHBG is high, total testosterone might appear adequate, while free testosterone is low, and the individual experiences symptoms. Conversely, with low SHBG, total testosterone might seem "too low," yet free testosterone remains normal, and no symptoms are present. Data from the large European study EMAS highlighted this discrepancy: men with normal total testosterone but low free testosterone (often older men with higher SHBG) exhibited deficiency symptoms, whereas those with low total testosterone but normal free testosterone (typically younger men with low SHBG) did not report an excess of such symptoms.
Practical takeaway: if total testosterone results fall into a gray area or don't align with symptoms, SHBG levels and calculated free testosterone provide more insight than a single number. An indicative threshold for deficiency has been proposed at calculated free testosterone below 220 pmol/l, though this recommendation is weak and remains under debate.
What Affects SHBG and Consequently Total Testosterone Interpretation
When SHBG is elevated, total testosterone can appear artificially high compared to the active fraction, making the results seem better than they actually are. Factors contributing to this include older age, hyperthyroidism, liver diseases, exposure to estrogens, caloric restriction, and malnutrition.
When SHBG is low, total testosterone might seem underestimated, even though free testosterone remains normal and symptoms may not be present. This can be caused by obesity, insulin resistance and type 2 diabetes, hypothyroidism, glucocorticoids and androgens, as well as metabolic syndrome.
How Sampling Conditions Affect Results
Testosterone isn't a fixed number written into your body forever. It follows a circadian rhythm, peaking in the morning. For younger men, up to one-third of the daily decline occurs within the first 30 minutes after waking up. In older men, this rhythm is flattened, but morning sampling remains the standard. Drawing blood in the afternoon can lower the result enough to place a healthy man near the "lower normal" range.
Your physical state at the time of the blood draw also matters. Eating a meal or consuming glucose can reduce testosterone levels, which is why endocrinologists recommend morning, fasting blood tests (urological guidelines are less strict about fasting but agree on the morning timing). A recent infection or other acute illness can temporarily lower levels, so testing isn't performed during a fever or immediately afterward.
The most important rule—and one that's easy to overlook. For nearly 30% of men with an initial result indicating a deficiency, a repeat measurement falls within the normal range. That's why a diagnosis can't be made based on a single test. At least two morning measurements are required, preferably taken on an empty stomach and when the individual is in a stable state of health.
Symptoms Truly Linked to Low Testosterone
Here's where the other half of the misunderstanding lies. Fatigue, low mood, and trouble concentrating are often associated with testosterone, but they are nonspecific: they can just as easily be explained by sleep deprivation, depression, hypothyroidism, anemia, chronic stress, or simple overwork. This combination of symptoms alone is a weak indicator of androgen deficiency.
The best indicators of low testosterone are three sexual symptoms identified in the EMAS study: reduced libido, erectile dysfunction, and the absence of morning erections. These form what is known as late-onset hypogonadism syndrome when they occur alongside biochemically confirmed deficiency. Importantly, erectile dysfunction can also be an early warning sign of vascular and cardiovascular diseases, so it shouldn't be immediately dismissed as "just a testosterone problem." Instead, it should prompt a broader look at overall health.
The rule is symmetrical. Low levels without symptoms and symptoms without confirmed low levels are not the same as a deficiency. Diagnosis requires meeting both conditions simultaneously: persistently low testosterone levels and corresponding symptoms.
How to Interpret Your Results in Practice
Before drawing conclusions from your lab report, consider a few key questions:
- When was the blood sample taken? Was it in the morning on an empty stomach, or in the afternoon after a meal? Was it a single measurement or a repeated one?
- What are the units and reference range of this lab? Is it ng/ml, ng/dl, or nmol/l, and what exact reference range has been adopted?
- Was only total testosterone measured? If the result falls in the gray zone or doesn't align with symptoms, it’s worth adding SHBG and free (calculated) testosterone to the analysis.
- Where does the value fall? Is it clearly low, in the gray zone of 8–12 nmol/l, or safely in the middle of the range?
- Do the symptoms match the results? Are there three sexual symptoms present, or is it more about nonspecific fatigue and low mood?
If the result is within the middle of the range, was taken in the morning, and you don’t have core sexual symptoms, testosterone is probably not the root cause of the issue, and it’s worth investigating other possibilities. However, if the value is in the gray zone or doesn’t align with clear symptoms, it’s a signal to deepen the diagnostics: repeat the measurement under proper conditions, add SHBG, free testosterone, and also LH, FSH, and prolactin, which help distinguish between testicular and pituitary causes. This diagnostic path should be followed with a doctor, ideally an endocrinologist or andrologist.
What not to do: don’t diagnose a deficiency based on a single number, don’t self-administer testosterone from an unknown source or use “boosters,” and don’t treat a supplement as a solution to a problem that hasn’t been confirmed yet. Unjustified testosterone therapy is not a neutral intervention—it affects, among other things, hematocrit levels and natural hormone production.
Key Takeaways
The "normal" range on a test result represents a statistical range, not a definitive threshold for health. Falling within it doesn't guarantee there's no issue, and being below it doesn't always indicate illness.
Diagnostic thresholds vary (AUA approximately 10.4 nmol/L, EAU 12 nmol/L), and between them lies a gray area where the number alone isn't conclusive.
Total testosterone doesn't reflect the active fraction. With atypical SHBG levels, only free testosterone provides an accurate picture.
Collection conditions affect results. Tests should be done in the morning, fasting, outside of acute illness, and repeated at least twice.
Results must be considered alongside symptoms. The most telling are three sexual symptoms; fatigue and mood changes are less specific.
Decisions rest with the physician. Interpretation, further diagnostics, and potential treatment are the responsibilities of an endocrinologist or andrologist, not for self-treatment.
Sources
European Association of Urology (EAU). Guidelines on Sexual and Reproductive Health, update 2024/2025 (threshold 12 nmol/l, free testosterone in the gray zone 8–12 nmol/l).
American Urological Association (AUA). Testosterone Deficiency Guideline (threshold 300 ng/dl; at least two morning measurements).
Bhasin S. et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab, 2018 (morning, fasting, repeated measurements; approximately 30 percent of results normalize upon retesting).
Wu FCW et al. Identification of Late-Onset Hypogonadism in Middle-Aged and Elderly Men. N Engl J Med, 2010 (EMAS study; three sexual symptoms).
Antonio L. et al. Low free testosterone and symptoms with normal total levels (EMAS analyses).
Antonio L. et al. Erectile dysfunction predicts mortality. Age and Ageing, 2022 (erectile dysfunction and morning erections versus mortality).
Handelsman D.J. et al. Accurate measurement of total and free testosterone levels for the diagnosis of androgen disorders. Best Pract Res Clin Endocrinol Metab, 2022 (importance of LC-MS/MS method and range discrepancies).